Last week, we hosted the first in our series of learning webinars, focusing on design considerations for inpatient settings.
We kicked off our first session - Lifesaving Considerations of Anti-barricade - looking back at the 2017 national safety alert for push button stops. We also reviewed the clinical feedback on operation and robustness that we continue to learn from throughout our design process.
A learning curve
It was a learning experience for us as much as it was for our delegates, in more ways than one. It was my first time hosting - a learning curve in itself - but we also gained a great deal of knowledge on the anti-barricade devices currently being used and the safety concerns that each raised.
During the webinar, we asked attendees to take part in a few polling questions to give us an understanding of their experiences of anti-barricade. The results were really interesting and highlight a number of things to look out for when you're assessing the suitability of anti-barricade doors and locks. So I thought I'd share them with you...
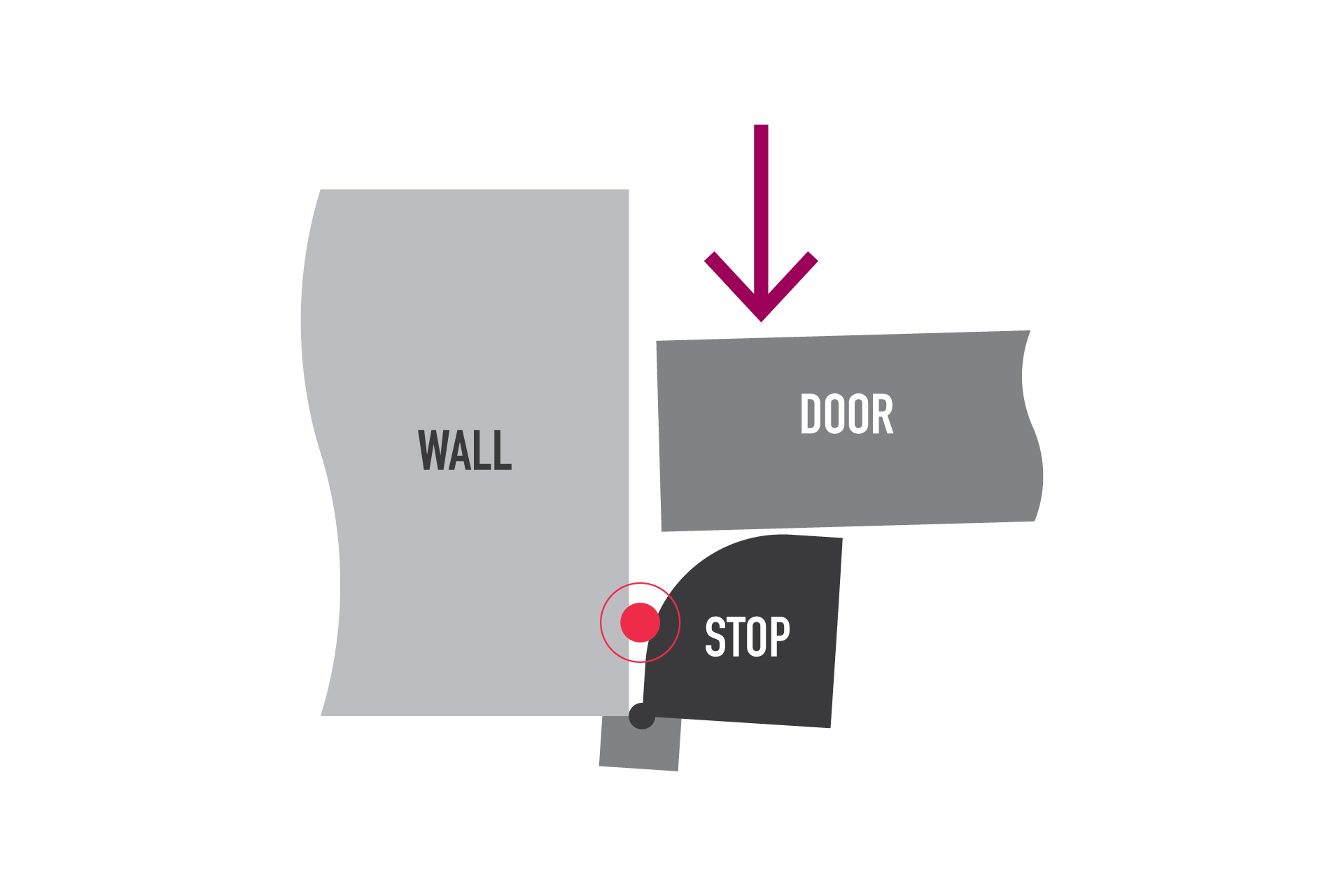
Push button stop
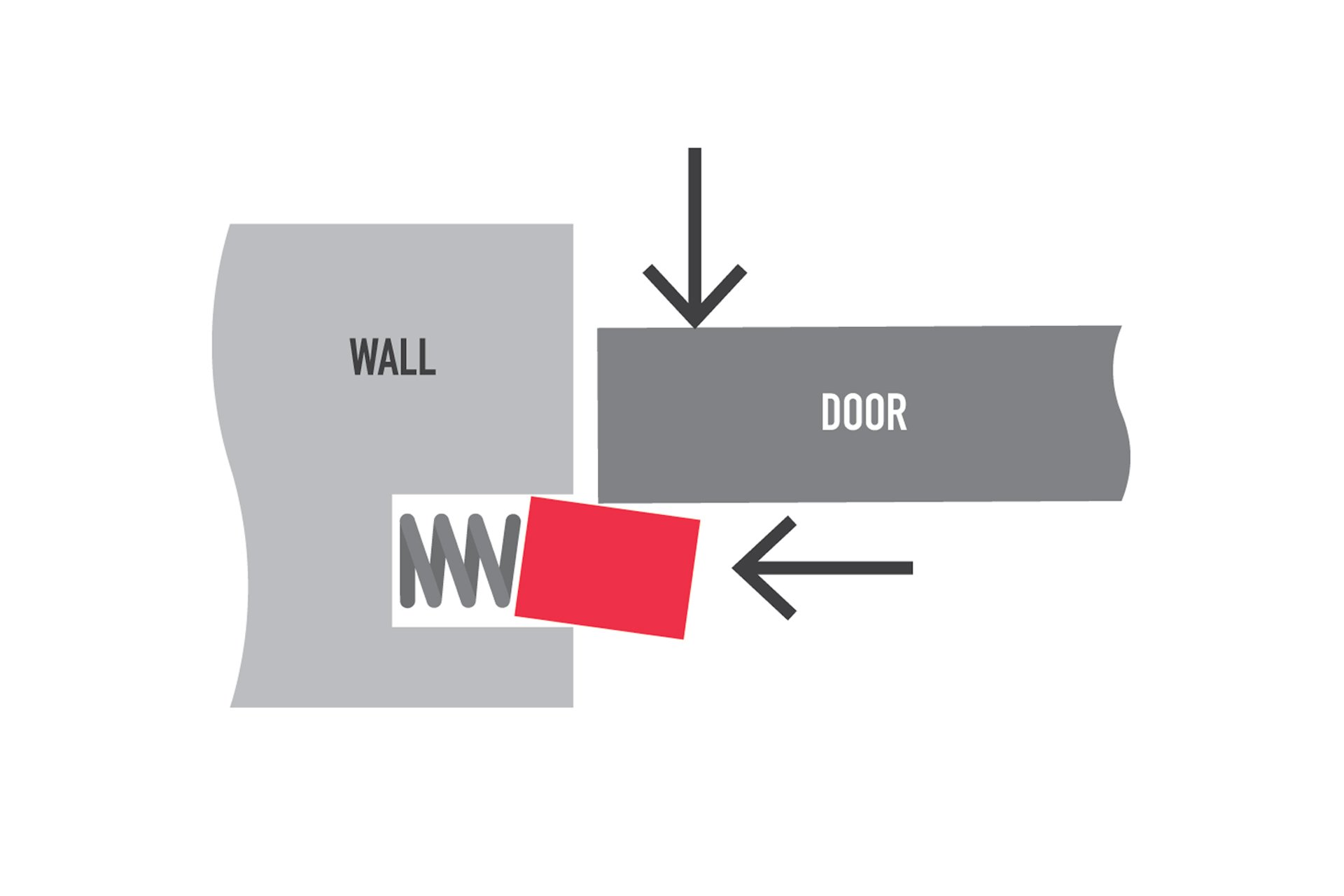
Push button stops were highlighted in the 2017 national safety alert
At 40%, our poll suggests that push button stops are still the most widely used anti-barricade device, despite the 2017 national safety alert questioning their efficacy. Those currently using push button stops reported difficulty operating under active force (32%), while 50% thought the stop looked institutional.
Double-articulated hinge
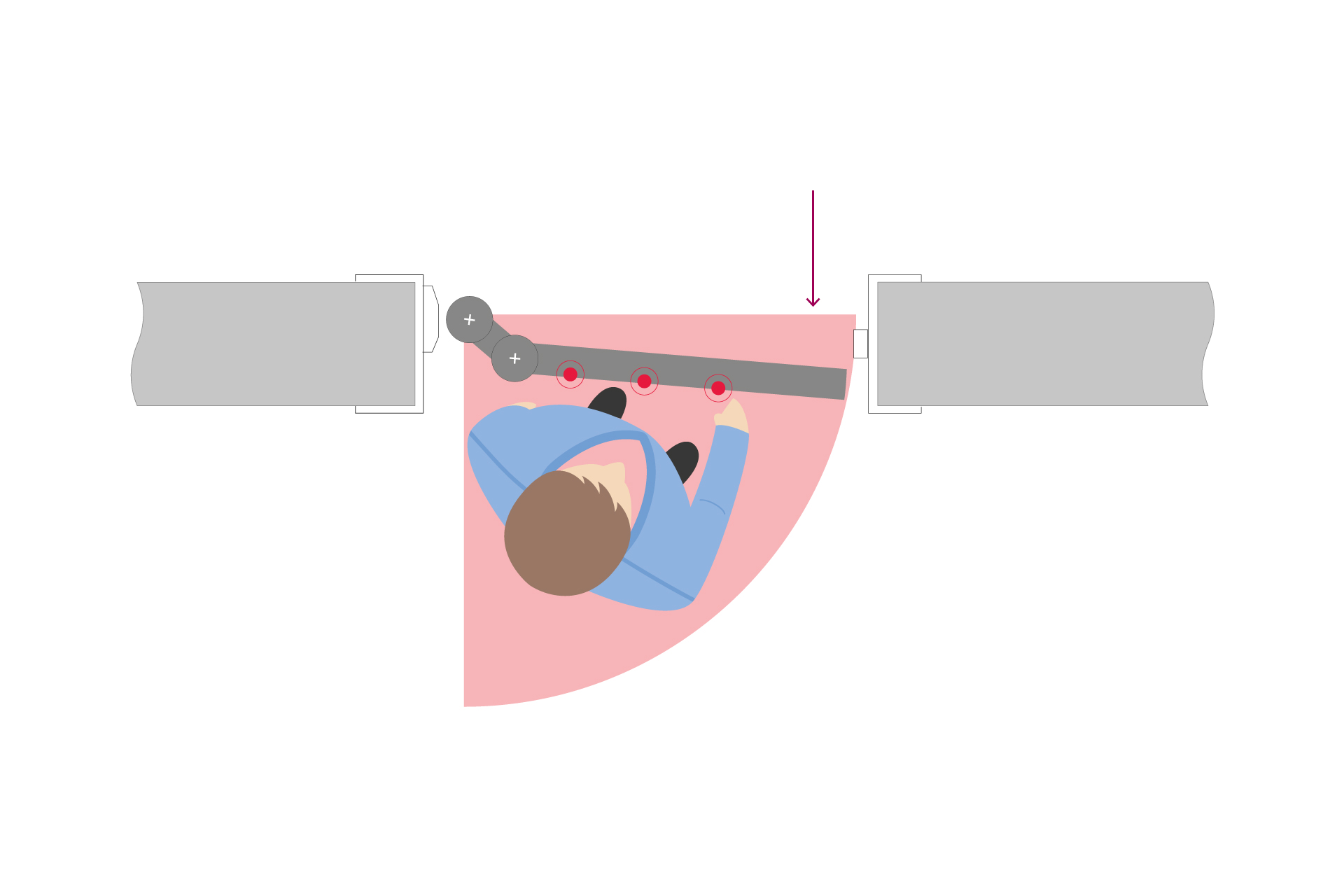
Double articulated hinges place staff directly in front of the door during operation
Another actively used alternative, and one of the newer solutions in recent years, 33% of our audience shared that they are currently using the double-articulated hinge. Within this group, 54% told us that they'd experienced damage to the point of failure.
The product also puts staff directly in front of the door; the most vulnerable location to be during a hostile barricade attempt. 31% also shared that the double-articulated hinge was complex to operate and needed staff training.
Removable door stop
Only 20% of our audience reported using the removable door stop. The main concern within this group was the length of time to access the room (67%).
Timber hinged stop
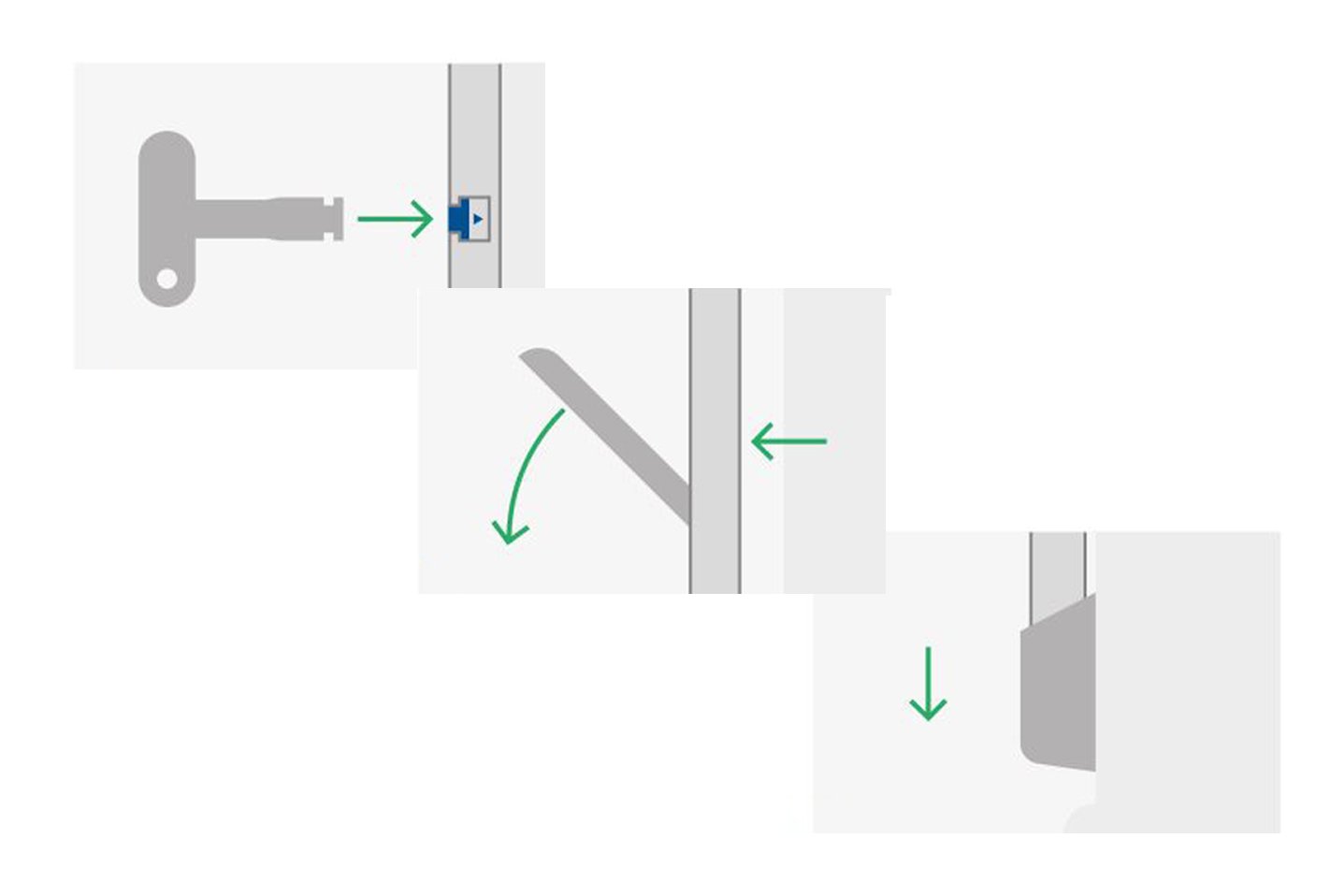
Clinical feedback highlights operational difficulty when internal pressure is applied
Less common among our audience was the timber hinged stop, with only 7% currently using it. In my experience, it's one of the most common solutions used in mental health environments, and perhaps the low response to the survey suggests people are already starting to move away from it. Complex operation was highlighted as their biggest concern.
Wider clinical feedback has highlighted that staff have personal safety concerns when using this product. They need to stand in front of the door and use the tip of their fingers to operate - making it very difficult when pressure is applied from the inside of the door.
The series continues...
A recording of the anti-barricade webinar is now available to watch on demand. Next in our series - Ligature and Self-harm Design Strategies - is set to take place on 28th May 2020.





